In the first of this two part series, I review the anatomy of the shoulder relevant to a labral tear. In the second part- Shoulder Labral Tear- Labral Repair and Rehabilitation, I review the current treatment strategy for a labral tear. With improvements in advanced imaging techniques, we are developing a better understanding of the functional role of different anatomic structures around the shoulder. This has helped us craft better therapeutic approaches and surgeries for damage such as a labral tear that may occur.
Anatomy
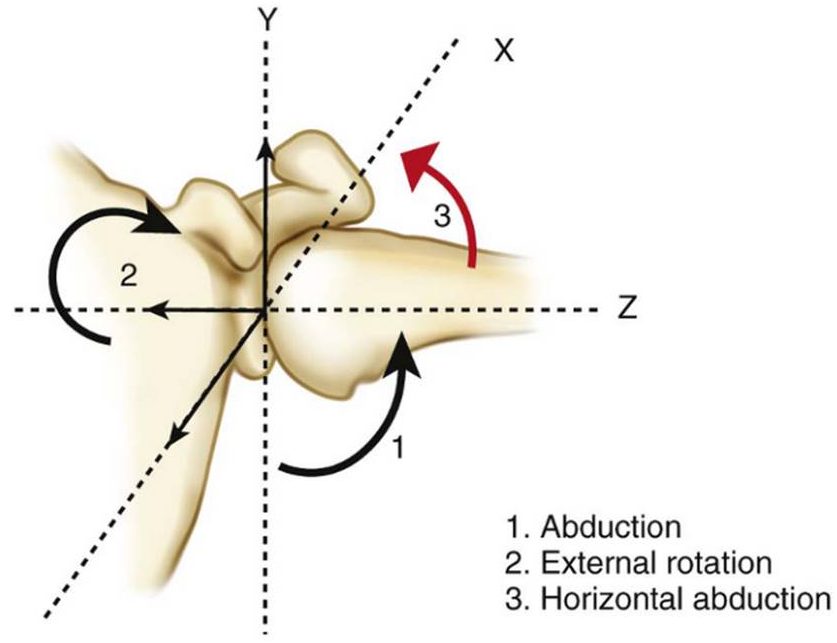
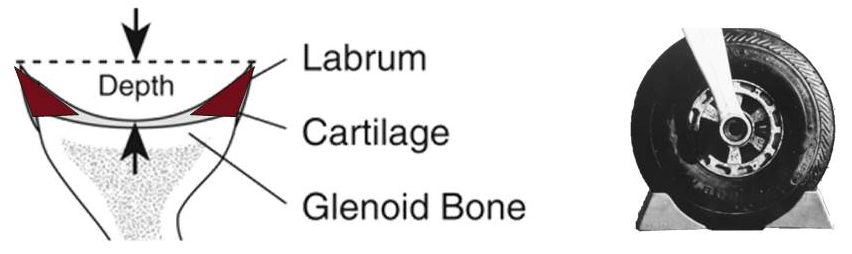
The shoulder is an amazingly mobile joint. It enjoys 6 degrees of freedom and helps us position our hand almost anywhere in space around our body. Thanks to the mobility of the shoulder we can both scratch our butt and comb our hair with the same arm! To achieve this motion, the shoulder relies on flexible soft tissue constraints to stabilize the shoulder joint. The shoulder joint has a ball and socket type configuration. The ball at the top of our upper arm, the humeral head, sits in a shallow bony socket, the glenoid. The humeral head is significantly larger than the overall size of the glenoid, with only 25% to 30% of the humeral head in contact with the glenoid at any given anatomic position. The bony glenoid concavity is quite shallow, with a depth of only a few millimeters.
“I often compare the bony anatomy of the shoulder joint to a golf ball sitting on a golf tee.”
In order to keep the “golf ball” on the “golf tee”, the shoulder relies on the surrounding soft tissue structures such as the muscles and ligaments to maintain the shoulder stability. One of the most important of these structures is the labrum. The labrum is like a rubber band that sits attached to the rim of the glenoid circumferentially encompassing the humeral head. Much like a chock block that prevents a wheel from rolling forward or backward, the labrum helps centralize the humeral head on the glenoid, and effectively deepen the socket.
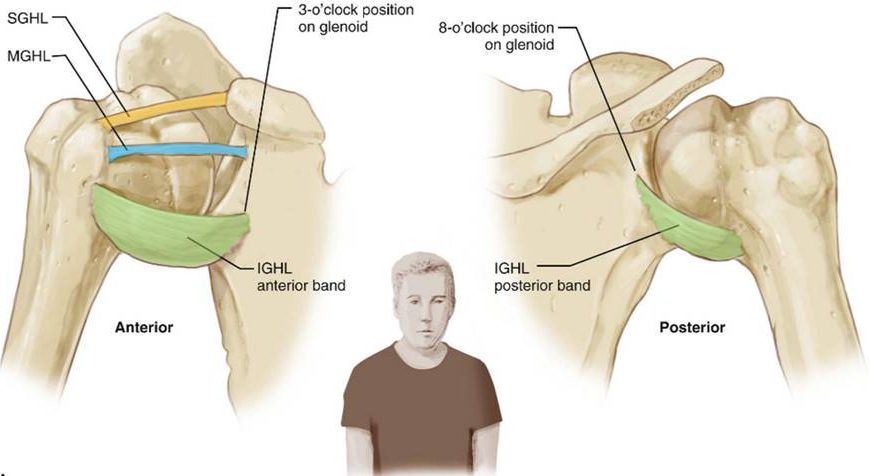
Surrounding the joint are several ligaments that help stabilize the joint. The glenohumeral ligaments and capsule that surround the shoulder joint also have roles in preventing excessive translation of the humeral head on the glenoid in any one specific direction. The four main glenohumeral ligaments are the superior glenohumeral ligament, the middle glenohumeral ligament, anterior inferior glenohumeral ligament, and posterior inferior glenohumeral ligament. Depending on the position of the shoulder, these ligaments provide varying degrees of constraint.
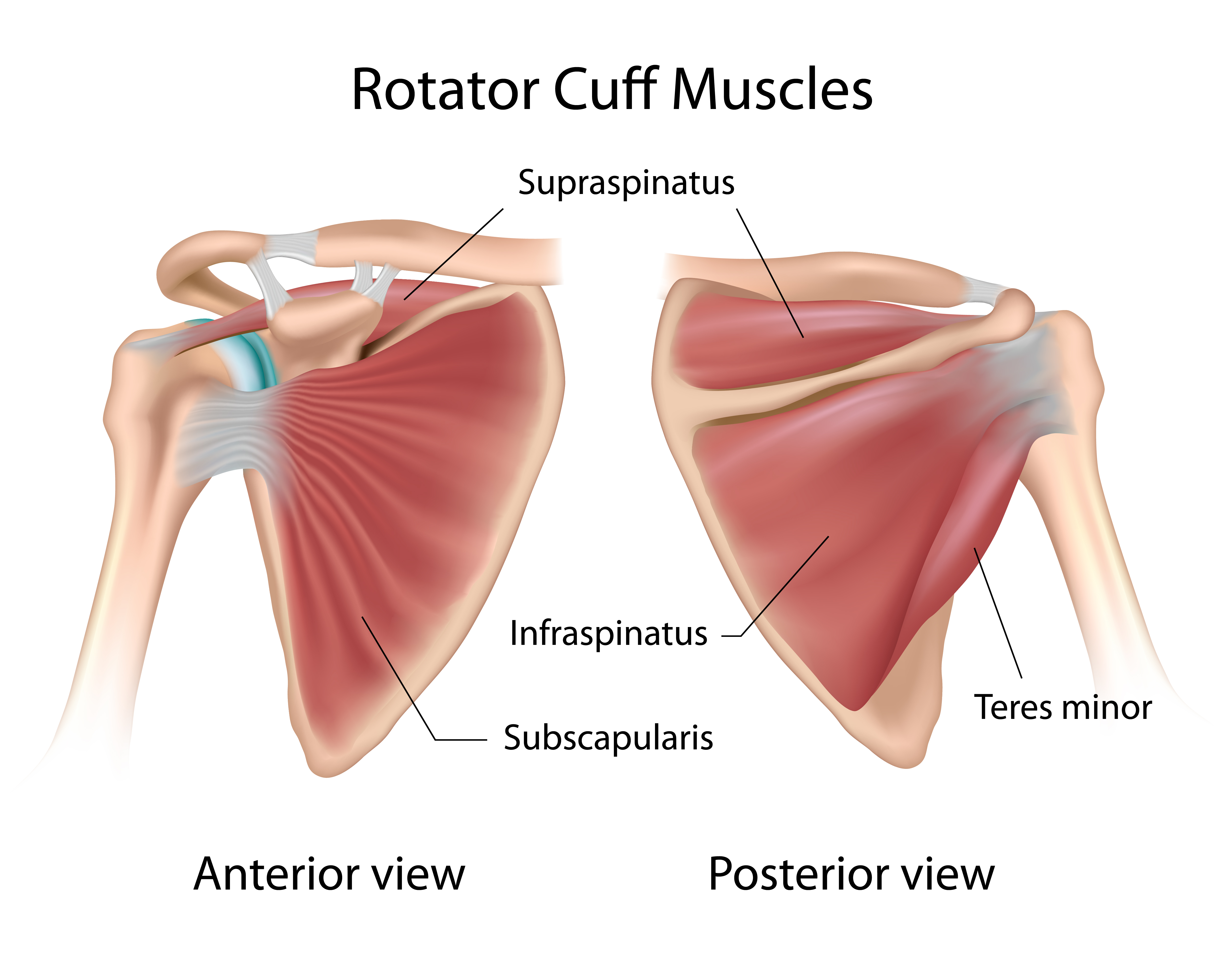
Finally the muscles surrounding or enveloping the shoulder joint, the rotator cuff muscles, provide a dynamic force for stabilization. Contraction of these muscles not only helps facilitate arm movement but hold the humeral head in the joint as it is moved. The four rotator cuff muscles are the subscapularis muscle, supraspinatus muscle, infraspinatus muscle, and teres minor muscle.
Function
Stability of a joint is a product of the constraining bony anatomy, supporting soft tissue ligaments, and surrounding muscle structure working together to permit stable movement. If any one of these components are compromised stability of the joint can be affected. Here we focus specifically on the role of the labrum and its importance in shoulder function. Certain injuries to the shoulder can cause a labral tear.
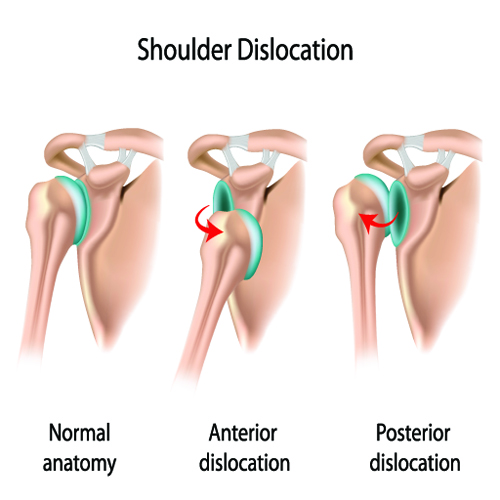
The most common mechanism for shoulder labral tear/damage is a shoulder dislocation. For a shoulder to dislocate out of the joint, something has got to give. That is at least one stabilizing structure must tear for the shoulder to slip out of the socket. Depending on one’s age certain structures are typically damaged. In the younger patient, usually the labrum around the humeral head tears. If the shoulder dislocates out the front, then the anterior inferior portion of the labrum is the most vulnerable to injury. This type of anterior inferior labral tear is called a Bankhart lesion. In contrast, in the older patient, the structure most likely to tear is the rotator cuff muscle. For an anterior dislocation supraspinatus or subscapularis tendon injury can be expected (you can learn more about rotator cuff tears here). A posterior shoulder dislocation behind the shoulder joint impacts the posterior labrum. In severe cases of trauma involving lots of energy, a combination of structures may get damaged such as the bony rim of the glenoid and/or the humeral head.
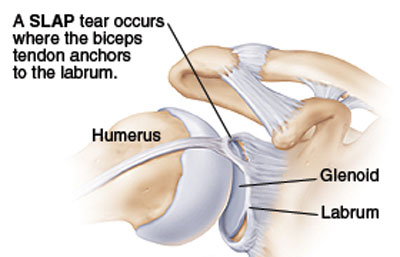
Another mechanism of labral damage involves overhead sports such as volleyball, baseball, raquetball, etc. High velocity and forceful movements of the arm such as those involved in pitching a baseball, or serving a tennis ball, can produce extreme forces across the shoulder. The labrum has an attachment to the biceps muscle that begins within the shoulder joint. As a result forces across the biceps muscle are imparted to the labrum where the two merge. This tension on the labrum can produce tears. These labral tears are called Superior Labral Anterior Posterior tears or SLAP tears due to their characteristic location adjacent to the biceps tendon in the shoulder joint. An acute labral tear from injury tends to be more problematic. A chronic attritional labral tear in contrast is often inconsequential.
Labral damage can also occur with a partial shoulder dislocation (also known as subluxation) or significant shoulder trauma after a fall. One common scenario is an injury to the labrum when lifting heavy weights overhead or during bench press. With heavy weights held far from the body, there is significant torque exerted across the shoulder joint. In this vulnerable position, the labrum can approach it’s mechanical capacity to maintain a stable shoulder, and consequently rupture if the forces exceed the physical limits of the labral tissue itself. Tears produced in the labrum this way are usually found in the posterior superior quadrant of the shoulder.
Labral Tear Diagnosis
Identifying labral damage on physical exam alone can be tricky. A high degree of suspicion based on the injury mechanism and history is necessary to direct a focused physical exam that attempts to provoke symptoms from the damaged labrum. Shoulder stability is a dynamic process and in some circumstances with minimal labral damage, a strong rotator cuff maybe adequate to maintain shoulder stability inspite of the labral damage. Symptoms from subtle labral damage can sometimes be the hardest to reproduce since symptoms are only elicited during the peak of shoulder performance during for example competitive sporting events.
MRI is the most effective way of confirming labral damage. A special type of MRI with an injection of contrasting dye into the shoulder is the most reliable way of detecting subtle labral damage. On imaging the radiologist or your orthopedist will look for damage to the structures that stabilize the shoulder. Separation or displacement of the labrum from the glenoid or shoulder socket can be readily noted. The rotator cuff is inspected carefully to ensure no damage. The glenoid and humeral head are also inspected closely to ensure any impaction or damage to the cartilage joint surfaces are detected.
Based on the damage detected, current functional level, and goals, the treatment is individually crafted.
Continue reading the second post in this series- Shoulder Labral Tear- Labral Repair and Rehabilitation, to learn more about the treatment of labral tears. If you suspect you may have a labral injury to your shoulder, call 281-690-4678 to make an appointment today for an individual consultation. A clear clinical history combined with a through physical exam can often give me much insight into the source of your dysfunction.
Sources:
http://orthoinfo.aaos.org/topic.cfm?topic=A00426
http://orthoinfo.aaos.org/topic.cfm?topic=A00035